Conduct a comprehensive eye and vision exam tailored for pediatric patients, focusing on visual function and early detection of serious pathology.
Visual Assessment
Evaluate the child's visual acuity using age-appropriate, child-friendly tools:
- Picture or symbol charts for pre-literate children.
- Snellen or similar letter charts for older children.
- Fixation and following behaviour in infants (does the child track a face or object?).
Visual acuity is often recorded as values such as 6/6 (or 20/20) if the child can see at a standard distance what is expected for normal vision. Use matching games, pointing, or picture naming for shy or non-verbal children.
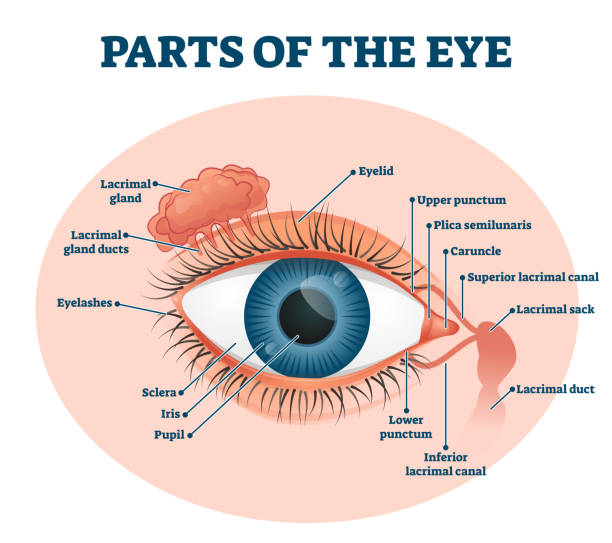
External Eye Examination
Inspect the peri-ocular region and anterior eye structures:
- Redness, swelling or discharge (conjunctivitis, blepharitis).
- Eyelids: ptosis, entropion/ectropion, incomplete closure.
- Lid position and movement: facial nerve palsy, poor blink.
- Lumps or bumps: chalazion, stye, masses.
- Foreign bodies: on conjunctiva, under lids, on cornea.
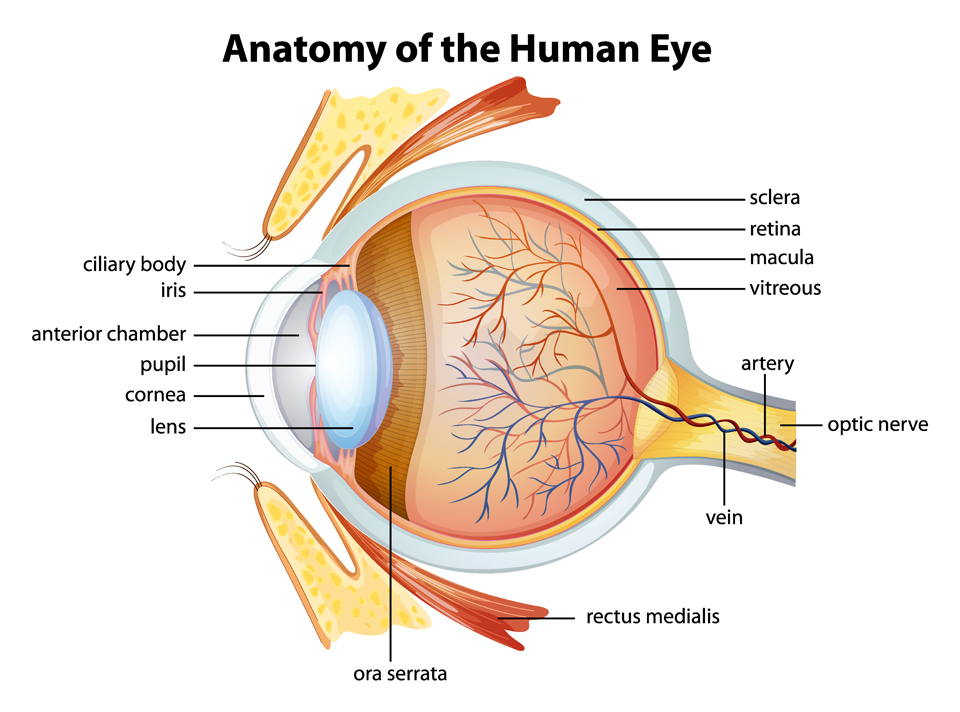
Internal Eye Examination
Use an ophthalmoscope and torchlight to assess:
- Pupillary response: Size, symmetry, direct and consensual light reflexes.
- Cornea: Clarity, scars, abrasions (consider fluorescein staining if corneal injury suspected).
- Lens: Clarity (look for cataract, leukocoria).
- Red reflex: Equal and bright in both eyes; any asymmetry or white reflex is concerning.
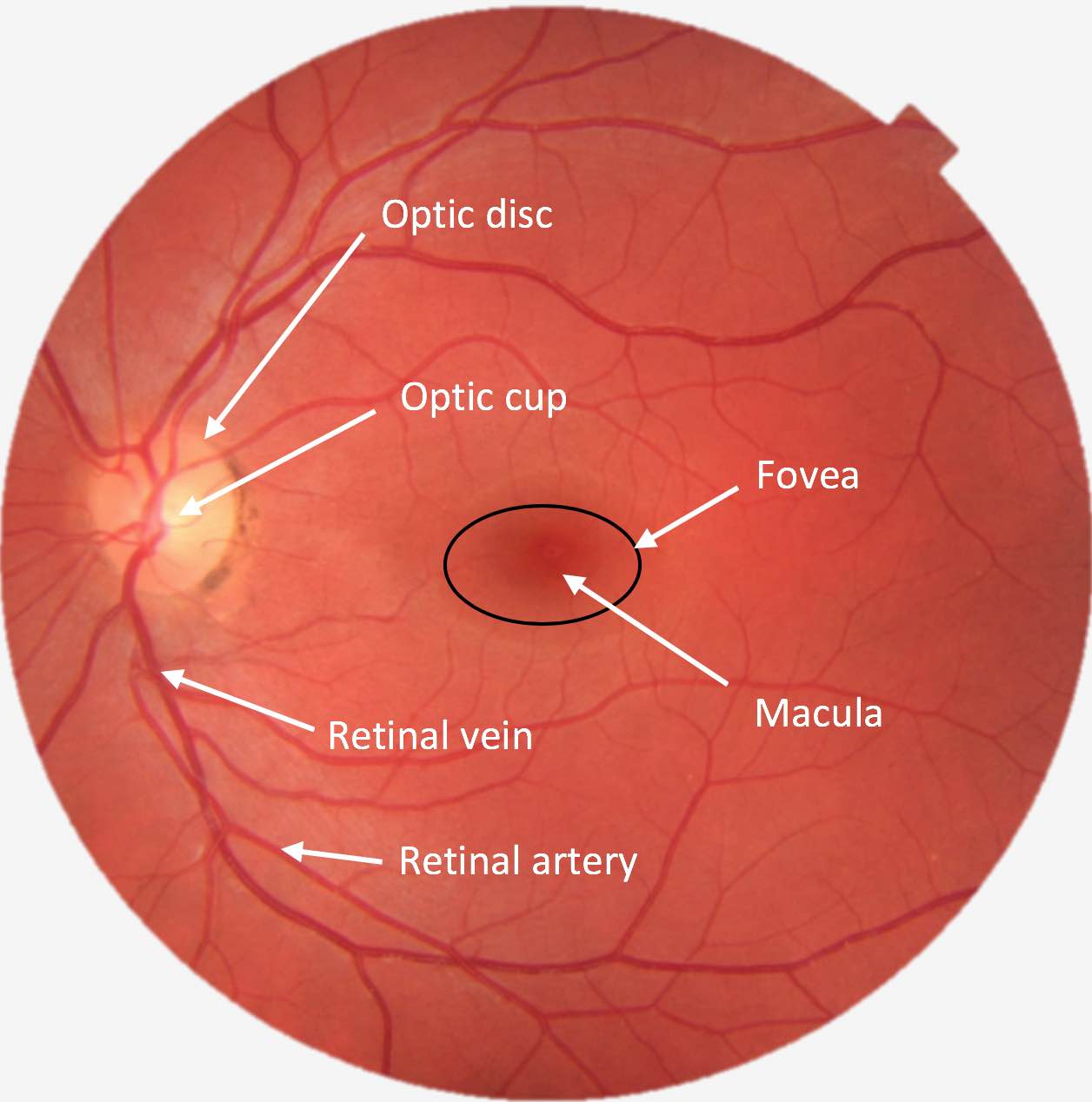
- Fundus (if possible): Optic disc, vessels, macula and background retina.
Intraocular Pressure
Measure intraocular pressure (IOP) with child-friendly methods (e.g. handheld tonometer) when indicated – such as suspected glaucoma or trauma. Note:
- Raised IOP may present with enlarged cornea, photophobia, tearing, irritability in infants.
- Always correlate with optic disc appearance and corneal findings.
Types of Pediatric Eye Conditions
| Type of Condition | Common Clinical Features |
|---|---|
| Amblyopia (Lazy Eye) |
|
| Conjunctivitis (Pink Eye) |
|
| Pre-septal Cellulitis |
|
| Orbital Cellulitis |
|
Pediatric Eye Red Flags
Any of the following should prompt urgent ophthalmology/senior review and often admission:
- Reduced visual acuity, especially acute onset or asymmetric vision.
- Leukocoria (white pupillary reflex) or abnormal red reflex.
- Severe eye pain or photophobia.
- Proptosis or obvious globe displacement.
- Painful or restricted eye movements.
- Marked eyelid swelling with systemic toxicity (concern for orbital cellulitis).
- History of high-velocity trauma, penetrating eye injury, or chemical exposure.
- New-onset strabismus, nystagmus, or abnormal eye movements.
- Associated neurological signs (headache, vomiting, seizures, altered consciousness).
- Infants who are persistently tearing, photophobic, and rubbing their eyes.
Quick Pediatric Eye Algorithm for A&E
Use this mental flow to structure assessment in the Emergency Department:
-
Initial Impression
- Is the child systemically unwell? (fever, toxic, septic picture)
- Is there any concern for orbital cellulitis, trauma, or chemical injury?
-
Check Vision and Red Flags
- Assess visual acuity in both eyes where possible.
- Look quickly for leukocoria, proptosis, corneal opacity, or marked swelling.
-
Define the Main Problem
- Red, sticky eye → conjunctivitis vs keratitis vs foreign body.
- Swollen eyelids → pre-septal vs orbital cellulitis.
- Painful, photophobic eye → consider keratitis, uveitis, acute glaucoma, corneal abrasion.
- Sudden visual change → urgent ophthalmology review.
-
Look for Red Flags
- If any red flag present → escalate for urgent imaging/ophthalmology input.
- If no red flags, child well, and likely minor condition → treat in ED and provide safety net advice.
-
Disposition
- Admit / urgent referral: orbital cellulitis, chemical injury, penetrating trauma, severe visual loss, suspected intra-ocular pathology.
- Discharge: mild conjunctivitis, simple corneal abrasion, stable pre-septal cellulitis on oral therapy (with good follow-up).
Common Pediatric Eye Emergencies
Key ophthalmic emergencies you will often encounter in A&E:
1. Orbital Cellulitis
- Swollen, red eyelids with proptosis, painful/restricted eye movements, decreased vision, fever.
- Medical emergency – risk of cavernous sinus thrombosis and intracranial spread.
- Urgent IV antibiotics, imaging (CT or MRI), and ophthalmology/ENT referral.
2. Pre-septal Cellulitis
- Eyelid swelling and redness without proptosis or pain on eye movement, and normal vision.
- Often associated with local skin infection or insect bite.
- Oral or IV antibiotics depending on severity and age; close follow-up.
3. Corneal Abrasion / Foreign Body
- Pain, photophobia, lacrimation, foreign body sensation.
- Examine with fluorescein; evert eyelids to look for hidden foreign body.
- Topical antibiotics, analgesia; avoid contact lenses until healed.
- Urgent referral if large central defects, suspected penetrating injury, or non-healing.
4. Chemical Eye Injury
- True emergency – start immediate irrigation before full history/exam.
- Irrigate with copious normal saline or clean water for at least 15–30 minutes.
- Check pH and repeat irrigation until normal.
- Urgent ophthalmology review after initial resuscitation and irrigation.
5. Acute Visual Loss
- Sudden reduction in vision in one or both eyes.
- Check acuity, pupils (RAPD), visual fields and fundus if possible.
- Urgent ophthalmology and possibly neurology referral – time-critical.
6. Leukocoria (White Pupil)
- Abnormal white reflex noticed by caregiver or on photos.
- Causes include cataract, retinoblastoma, retinal detachment, Coats disease.
- Requires urgent specialist assessment – treat as high priority.
Always document visual acuity (or best possible assessment), red reflex, key findings, and safety net advice clearly in the notes.